
A 66-Year-Old Man With Potential Bleeding Complications: Is Surgery Still an Option?
Correct Answer: C. The patient's most likely diagnosis is an acquired anti-coagulant of lupus type (lupus inhibitor).
Discussion. A patient opting for elective surgery had an abnormal clotting test, namely an isolated, impressive prolongation of the PTT. Beside the abnormal test itself, an important question must be asked: will the abnormality result in bleeding risk with surgery?
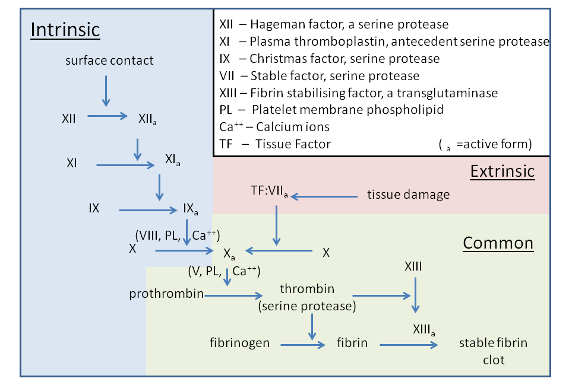
There is no better way to explain the clotting tests than with the classical schematic of the coagulation cascade,1 wherein the liquid plasma has proteins which enzymatically activate each other in cascade fashion with the result being a fibrin clot capable of searing off wounds in blood vessels and therefore stopping bleeding (Figure 1).

Fig. 1. A visual example of the coagulation cascade is shown. CC BY-SA 3.0. Image courtesy of Dr Graham Beards.The commonly used screening coagulation tests add a stimulating agent to the plasma specimen that can initiate one of these cascades and measuring the time required for a fiibrometer to detect the formation of an insoluble fibrin clot.
For a PTT, a tissue thromboplastin capable of activating Factor XII is added, which fires down the "intrinsic pathway" to form a fibrin clot within 26-36 seconds. For the prothrombin time, a tissue extract, often bovine brain extract, capable of activating Factor VII, is added to plasma, which then fires down the "extrinsic pathway" to form a fibrin clot within 10-13 seconds. Note that when combined, the prothrombin time (PT) and PTT act as controls for each other in that if either is normal there is localization to the proteins in the abnormal pathway.
In the present patient, the PTT is abnormal, yet the PT is within normal limits, thus isolating the problem to one of the proteins in the intrinsic arm. This is far more common than isolated prolongation of the extrinsic pathway. Indeed, in most instances, affecting the extrinsic pathway also impacts the PTT such as severe liver disease and warfarin anticoagulant medicines, which lower not just Factor VII (extrinsic pathway) but also Factors IX, X, and XI in the intrinsic pathway arm.
Clinical experience and data analysis have yielded important clinical parameters to guide algorithms for evaluating and definitively diagnosing the causation of isolated prolonged PTT. The following historical factors need be considered:
- inpatient or outpatient setting;
- any prior history for presence of prolonged PTT;
- any history of unusual bleeding, spontaneous or with surgery/trauma; and
- whether the patient is currently bleeding or was recently bleeding.2
Dealing with these strong clinical clues, in-patient PTT prolongation raises the distinct possibility of exposure to therapeutic or prophylactic anticoagulants usually in the heparin family. Repeating the PTT after adding heparinase (a heparin degrading enzyme) will frequently normalize the PTT and provide the answer. A prior history of unusual bleeding with trauma, with surgery, at delivery, or with the extraction of permanent teeth is a strong clue to the presence of "mild hemophilia" with levels of either intrinsic factors VII, IX, or XI below normal. This may be adequate for everyday life, but it is not adequate for hemostatic stress situations. These patients will bleed in such circumstances. There is no such thing as mild hemophilia with trauma or surgery.
Most patients with mild hemophilia will manifest a baseline prolongation of PTT, often not impressively high but still prolonged (37-45 seconds) if the test had ever previously been performed. This is the scenario offered in Answer B and does not fit the findings in the case presentation.
When a patient with no previous bleeding history and a previously known normal PTT is bleeding (either spontaneously or while experiencing hemostatic stress), spontaneous acquired Factor VIII deficiency due to autoimmune antibody specific to Factor VIII is likely. This dangerous condition (excess of 50% mortality) is seen most often in geriatric populations (80 years of age or older) and causes profuse, diffuse, often life-threatening bleeding with spreading ecchymoses/hematoma formation, mucosal bleedings, and internal organ hemorrhages. Therapeutics are quite difficult and require refined laboratory, blood bank, and specialist availability and involvement.3 This is the situation offered in Answer A, which was not how our case was behaving.
Finally, there is the situation like our present case with entirely negative bleeding history despite background of surgery. Our patient has previously had normal coagulation testing and no recent or active bleeding, yet he is manifesting a quite prolonged PTT. Our patient is most likely dealing with a lupus-type anticoagulant. This is an acquired antibody that binds to phospholipids (as with other anti-cardiolipin syndromes) and interferes with and prolongs the PTT test in vitro. But in vivo, the lupus-type anticoagulant does not produce abnormal bleeding. In fact, paradoxically these antibodies correlate with increased thrombotic risk in this patient population.2,4
A specific diagnosis requires a series of coagulation testing probing the coagulation cascade. Testing includes a thrombin time wherein preformed thrombin is added to plasma. If prolonged, an anti-thrombin is present (usually a heparin or non-vitamin K oral anticoagulants as previously discussed). If the PT is normal, then vitamin K antagonists and liver disease are excluded, and the abnormality is localized to the Intrinsic coagulation cascade.
The key test is then the mixing study, where 50% of normal plasma is mixed with 50% patient plasma and a PTT is performed. If there is correction, then factor deficiency of either XII, IX, VIII, or IX is present and further specific measurements of these factors will make a definitive diagnosis. If there is no correction, then one of these two situations remain, namely acquired specific antibody almost always against Factor VIII ("acquired hemophilia") or there an autoimmune anti-phospholipid anticoagulant antibody ("lupus type inhibitor") is present. Clinically, a patient with the former will almost always be recently, currently, and significantly bleeding. While in the latter, a patient bleeds not at all in history or in person. Specific antibody and coagulation testing will confirm, which of these two are present, although the different clinical scenarios will merely confirm what is suspected.
Patient follow-up. A series of laboratory tests were performed on the patient. A routine coagulation panel confirmed the initial studies with PT 13 seconds/INR 1.0 and the PTT again at 85 seconds. This excluded technical issues such as dilution in the original testing. A thrombin time was normal as was a heparinase study, which excluded the presence of antithrombin medicine. Simultaneously, Factor VIII level and lupus anticoagulant testing was performed and revealed Factor VIII level of 96% (normal 51%-110%) and the confirmed presence of a lupus type anticoagulant consistent with the total absence on bleeding in the history.
The patient proceeded with elective elbow surgery with no excessive bleeding complications. The physicians were aware of the thrombosis risk in lupus anticoagulant patients. However, because the procedure was outpatient and less than 1 hour of anesthesia with immediate ambulation and return to normal activity, no additional thromboprophylaxis was used. He was well 2 weeks post-operation. He'll be followed at intervals to monitor whether the lupus anticoagulant persists as well as the potential onset of new symptoms related to it.
What’s the take home? Since many patients undergoing surgery of all kinds are "screened" for bleeding risk (platelet count and PTT, on occasion) an unexpected abnormality will occur. The so-called "isolated prolonged PTT" is one such situation. A very expedited and classic evaluation based upon clinical findings and coagulation testing is used to specifically diagnose the cause in these cases. Clinical criteria include:
- whether the patient is inpatient or outpatient¾ inpatients often have been exposed to antithrombin medicines such as heparin;
- whether the patient is an adult or child¾children/infants have different potential diagnoses and their frequencies; and
- any lifetime history and recent history of abnormal bleeding either with trauma, surgeries, dental extractions, or spontaneously.
Specific coagulation testing uses thrombin time and heparinase to exclude the presence of antithrombin medications, a mixing study to exclude mild subclinical factor deficiency, and the presence of an inhibitor. Finally, a differentiation of specific antibody to Factor VIII or the presence of a lupus type anti-phospholipid anticoagulant separates these two types of inhibitors. Clinically, they present very differently¾ specific Factor VIII inhibitors bleed a great deal, while lupus type anti-coagulants rarely or ever do so.
The presence of a lupus anticoagulant is not a bleeding risk, and patients can proceed with planned and required procedures without supportive therapy. In fact, the presence of a lupus type anticoagulant is more of a thrombotic risk, more so than the presence of anticardiolipin antibodies alone so perioperative prophylaxis is an important consideration in such patients.4
AUTHOR
Ronald N. Rubin MD1,2AFFILIATIONS
1Lewis Katz School of Medicine at Temple University, Philadelphia, PA
2Department of Medicine, Temple University Hospital, Philadelphia, PACITATION
Rubin RN. A 66-Year-Old Man With Potential Bleeding Complications: Is Surgery Still an Option? Consultant. 2024;65(4):10.25270/con.2025.04.000002DISCLOSURES
The author reports no relevant financial relationships.CORRESPONDENCE:
Ronald N. Rubin, MD, Temple University Hospital, 3401 N. Broad Street, Philadelphia, PA 19140 (blooddocrnr@yahoo.com)References
- Kamal AH, Tefferi A, Pruthi RK. How to interpret an abnormal prothrombin time, activated partial thromboplastin time, and bleeding time in adults. Mayo Clin Proc. 2007;82(7):864-873.
- Tchernintchouk O, Laposato M, Marque MB. The isolated prolonged PTT. Am J Hematol. 2013;80(1):62-65.
- Kruse-Jarres R, Leissinger CA. Acquired coagulation disorders caused by inhibitors. In: Kitchen CS, Kessler CM, Konkle BA, eds. Consultative Hemostasis and Thrombosis. 3rd ed. Elsevier-Saunders; 2013:79-89.
- Galli M, Luciani D, Bertolini G, Barbui T. Lupus anticoagulants are stronger risk factors for thrombosis than anticardiolipin antibodies in the antiphospholipid syndrome: a systematic review of the literature. Blood. 2003;101(5):1827-1832.
©2025 HMP Global. All Rights Reserved. Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Consultant360 or HMP Global, their employees, and affiliates.
{kind=link}