
An Atlas of Lumps and Bumps, Part 50: Maculopapular Cutaneous Mastocytosis
Maculopapular Cutaneous Mastocytosis
Maculopapular cutaneous mastocytosis (also known as urticaria pigmentosa) is the most common form of cutaneous mastocytosis and accounts for 70% to 90% of pediatric cases.1-3 Its incidence has been estimated to be 1 in 150,000.4 Approximately 80% of cases occur within the first year of life.5-7 Congenital cases have been described in 15 to 25% of patients.5,8 The sex ratio is approximately equal.3,5,8 The condition is more commonly reported in Caucasian patients.3,10 The majority of cases occur sporadically.3,5,11 Familial cases have also been reported.11,12 An autosomal dominant mode of inheritance with incomplete penetrance has been described.13
Two main clinical variants of maculopapular cutaneous mastocytosis have been recognized: polymorphic and monomorphic.14 The polymorphic variant is most common and seen mainly in children11 (Figure 1).
Fig. 1. The polymorphic maculopapular cutaneous mastocytosis variant is generally seen in children.
This variant typically present with pruritic, polymorphic erythematous to reddish-brown macules or papules of different sizes and shapes (Figure 2).1

Fig. 2 The polymorphic maculopapular cutaneous mastocytosis variant present with pruritic, polymorphic erythematous to reddish-brown macules or papules of different sizes and shapes.
Lesions can be few (≥ 4) or numerous and are larger than those seen in the monomorphic variant as well as the adult-onset maculopapular cutaneous mastocytosis.1,4,15,16 (Figure 3).
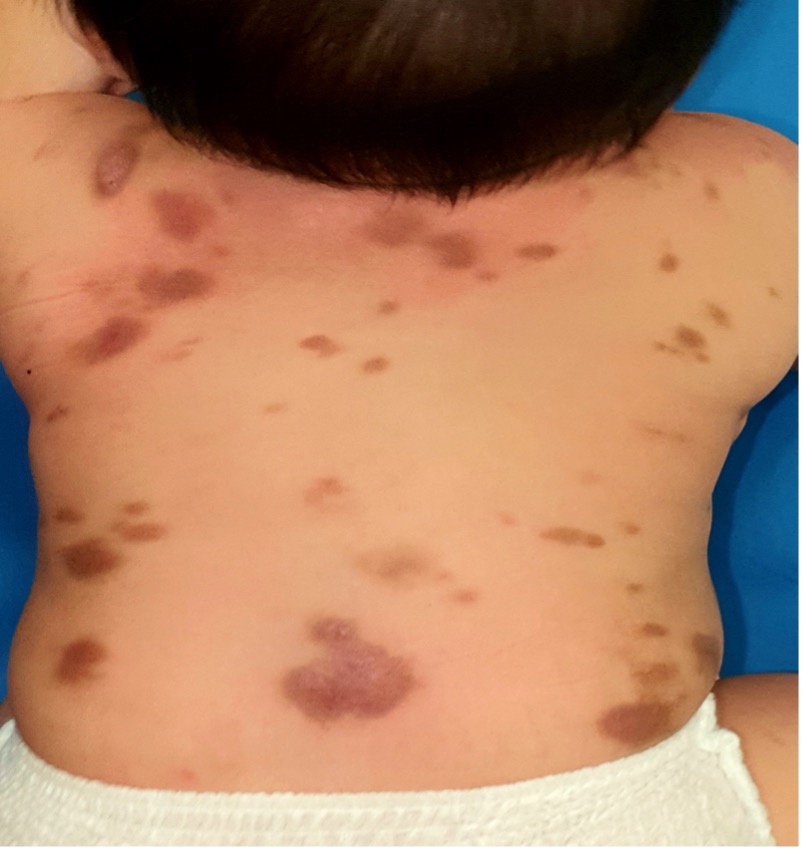
Fig. 3. Lesions can be few (≥ 4) or numerous and are larger than those seen in the monomorphic variant.
The margins can be sharp or indistinct.1 Sites of predilection include the trunk and proximal extremities.3,6,17 The palms, soles, face and scalp are usually spared.6,14 The lesions may spontaneously urticate and/or urticate when stroked or rubbed (Darier sign) (Figure 4); this sign is pathognomonic of mastocytosis.4,14
Fig. 4. The lesions may spontaneously urticate and/or urticate when stroked or rubbed (Darier sign).
Pruritus is the most common symptom.2,6 Dermographism is often present.1 Flares usually manifest as lesional erythema, edema, and intense pruritus.1,3 Although flushing is more commonly seen in patients with systemic mastocytosis, flushing occurs in 17 to 36% of patients with maculopapular cutaneous mastocytosis.17 Systemic symptoms such as pruritus, flushing, blistering, dizziness, palpitations, abdominal pain, diarrhea, and syncope are more common in children with greater skin involvement and higher tryptase level.18 Organomegaly and lymphadenopathy are characteristically absent.
A small number of children with maculopapular cutaneous mastocytosis present with numerous small monomorphic round lesions where all lesions are similar in size, shape and color.4,14,17 This variant is more commonly seen in adult-onset maculopapular cutaneous mastocytosis. (Figure 5).15,16

Fig. 5. Although rare, some children with maculopapular cutaneous mastocytosis present with numerous small monomorphic round lesions where all lesions are similar in size, shape and color.
In contrast to those children with large polymorphic lesions who have the onset of disease usually during infancy, children with small monomorphic round lesions usually have the onset of disease after the age of 2 years.9
Other rare clinical variants include bullous form, nodular, plaque, and xanthelasmoid forms, diffuse erythrodermic mastocytosis and telangiectasia macularis eruptiva perstans.6,14,19,20
The diagnosis is mainly clinical, based on the morphology of lesions and the presence of a positive Darier sign. Dermoscopy typically shows a light-brown blot, brown reticular lines, and a pigmented network that corresponds to the accumulation of melanin in basal keratinocytes.21-23 The diagnosis can be confirmed, if necessary, by a skin biopsy that confirms infiltrate of mast cells in the dermis and demonstration of KIT mutation in lesional skin.14
The prognosis for this condition is good.11 Most children with the polymorphic variant have spontaneous resolution of the lesions before puberty.2,6,14 In one study, the mean duration of the disease was 10 years.24 On the other hand, children with the monomorphic variant tend to have persistence of the lesions until adulthood and may have systemic involvement in other organs.2,6,14 In one study, only 1.9% of these cases resolved each year.25 Adult-onset maculopapular cutaneous mastocytosis has a much higher chance of progression to systemic disease.1
AUTHORS:
Alexander K.C. Leung, MD1,2, Benjamin Barankin, MD3, Joseph M. Lam, MD4, Kin Fon Leong, MD5
AFFILIATIONS:
1Clinical Professor of Pediatrics, the University of Calgary, Calgary, Alberta, Canada
2Pediatric Consultant, the Alberta Children’s Hospital, Calgary, Alberta, Canada
3Dermatologist, Medical Director and Founder, the Toronto Dermatology Centre, Toronto, Ontario, Canada
4Associate Clinical Professor of Pediatrics, Dermatology and Skin Sciences, the University of British Columbia, Vancouver, British Columbia, Canada.
5Pediatric Dermatologist, the Pediatric Institute, Kuala Lumpur General Hospital, Kuala Lumpur, Malaysia
CITATION:
Leung AKC, Barankin B, Lam JM, Leong KF. An Atlas of Lumps and Bumps, Part 50: Solitary Cutaneous Mastocytoma. Consultant. 2025;65(4):10.25270/con.2025.04.000003.
CORRESPONDENCE:
Alexander K. C. Leung, MD, #200, 233 16th Ave NW, Calgary, AB T2M 0H5, Canada (aleung@ucalgary.ca)
EDITOR’S NOTE:
This article is part of a series describing and differentiating dermatologic lumps and bumps. To access previously published articles in the series, visit: https://www.consultant360.com/resource-center/atlas-lumps-and-bumps.
References
- Leung AKC, Barankin B. What is causing this skin eruption? Urticaria pigmentosa. Consult Pediatr. 2016;15:311-313.
- Barnes M, Van L, DeLong L, Lawley LP. Severity of cutaneous findings predict the presence of systemic symptoms in pediatric maculopapular cutaneous mastocytosis. Pediatr Dermatol. 2014;31(3):271-275. doi:10.1111/pde.12291
- Mir A, Chamlin SL. A 1-year-old boy with persistent, generalized eruption. Urticaria pigmentosa. Pediatr Ann. 2014;43(1):e13-e15. doi:10.3928/00904481-20131223-11
- Hartmann K, Escribano L, Grattan C, et al. Cutaneous manifestations in patients with mastocytosis: consensus report of the European Competence Network on Mastocytosis; the American Academy of Allergy, Asthma & Immunology; and the European Academy of Allergology and Clinical Immunology. J Allergy Clin Immunol. 2016;137(1):35-45. doi:10.1016/j.jaci.2015.08.034
- Brockow K. Urticaria pigmentosa. Immunol Allergy Clin North Am. 2004;24(2):287-316. doi:10.1016/j.iac.2004.01.002
- Castells M, Akin C. Mastocytosis (cutaneous and systemic): epidemiology, pathogenesis, and clinical manifestations. In: Post TW, ed. UpToDate. Waltham, MA. Accessed March 17, 2021.
- Castells M, Akin C. Mastocytosis (cutaneous and systemic): Evaluation and diagnosis in children. In: Post TW, ed. UpToDate. Waltham, MA. Accessed March 17, 2021.
- Tuysuz G, Ozdemir N, Apak H, et al. Childhood mastocytosis: result of a single center. Turk Pediatr Ars. 2015;50(2):108-113. doi:10.5152/tpa.2015.2332
- Wiechers T, Rabenhorst A, Schick T, et al. Large maculopapular cutaneous lesions are associated with favorable outcome in childhood-onset mastocytosis. J Allergy Clin Immunol. 2015;136(6):1581-1590.e3. doi:10.1016/j.jaci.2015.05.034
- Cowart D, Cowart K, Hougeir FG. A 39-year-old woman with spots covering her body. BMJ Case Rep. 2013;2013:bcr2013201434. doi:10.1136/bcr-2013-201434
- Yavuz GO, Yavuz IH, Bilgili SG, et al. Urticaria pigmentosa in monochorionic twins. Indian J Dermatol Venereol Leprol. 2019;85(5):509-511. doi:10.4103/ijdvl.IJDVL_163_18
- Azana JM, Torrelo A, Matito A. Update on mastocytosis (part 1): pathophysiology, clinical features, and diagnosis. Actas Dermosifiliogr. 2016;107(1):5-14. doi:10.1016/j.ad.2015.09.007
- Fett NM, Teng J, Longley BJ. Familial urticaria pigmentosa: report of a family and review of the role of KIT mutations. Am J Dermatopathol. 2013;35(1):113-116. doi:10.1097/DAD.0b013e31826330bf
- Di Raimondo C, Del Duca E, Silvaggio D, et al. Cutaneous mastocytosis: A dermatological perspective. Australas J Dermatol. 2021;62(1):e1-e7. doi:10.1111/ajd.13443
- Macri A, Cook C. Urticaria pigmentosa. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan–. PMID: 29494109.
- Matito A, Azaña JM, Torrelo A, Alvarez-Twose I. Cutaneous mastocytosis in adults and children: New classification and prognostic factors. Immunol Allergy Clin North Am. 2018;38(3):351-363. doi:10.1016/j.iac.2018.04.001
- Allison MA, Schmidt CP. Urticaria pigmentosa. Int J Dermatol. 1997;36(5):321-325. doi:10.1046/j.1365-4362.1997.00029.x
- Gurnee EA, Johansen ML, Phung TL, et al. Pediatric maculopapular cutaneous mastocytosis: Retrospective review of signs, symptoms, and associated conditions. Pediatr Dermatol. 2021;38(1):159-163. doi:10.1111/pde.14399
- Choudhary S, Srivastava A, Joshi D, Tummudi S. Localized grain-leather plaque in urticaria pigmentosa—An unusual coexistence of dual morphology. Indian Dermatol Online J. 2020;11(5):796-798. doi:10.4103/idoj.IDOJ_540_19
- Panigrahi A, Chakraborty S, Sil A. Urticaria pigmentosa. J Pediatr. 2020;222:249. doi:10.1016/j.jpeds.2020.03.053
- Chauhan P, Bhardway N, Shirazi N. Dermoscopy of urticaria pigmentosa. Indian Dermatol Online J. 2020;11(3):475-476. doi:10.4103/idoj.IDOJ_438_18
- Miller MD, Nery NS, Gripp AC, Maceira JP, Nascimento GM. Dermatoscopic findings of urticaria pigmentosa. An Bras Dermatol. 2013;88(6):986-988. PMID:24474113.
- Nirmal B, Krishnaram AS, Muthu Y, Rajagopal P. Dermatoscopy of urticaria pigmentosa with and without Darier's sign in skin of colour. Indian Dermatol Online J. 2019;10(5):577-579. doi:10.4103/idoj.IDOJ_501_18
- Heinze A, Kuemmet TJ, Chiu YE, Galbraith SS. Longitudinal study of pediatric urticaria pigmentosa. Pediatr Dermatol. 2017;34(2):144-149. doi:10.1111/pde.13066
- Le M, Miedzybrodzki B, Olynych T, Chapdelaine H, Ben-Shoshan M. Natural history and treatment of cutaneous and systemic mastocytosis. Postgrad Med. 2017;129(8):896-901. doi:10.1080/00325481.2017.1364124