
Continuous Adductor Canal Catheter Offers Pain Relief Benefits But No Opioid-Sparing Advantage After Knee Replacement
Key Highlights
- No statistically significant reduction in opioid consumption was observed between catheter and single-shot adductor canal block (ACB) groups during the 24 to 48-hour postoperative period.
- The catheter group experienced significantly lower rest pain scores on postoperative day 2 and required less rescue intravenous opioids.
- Opioid-related side effects were fewer in the catheter group on postoperative day 2.
In a randomized controlled trial involving 94 patients undergoing total knee arthroplasty (TKA), extending the adductor canal block (ACB) with a continuous catheter did not reduce opioid consumption in the 24 to 48-hour postoperative period compared with a single-shot ACB with perineural dexamethasone. However, patients in the catheter group reported significantly lower pain at rest on postoperative day 2 and exhibited reduced usage of rescue intravenous opioids as well as fewer opioid-related side effects. The study authors presented their results at the 50th Annual Regional Anesthesiology and Acute Pain Medicine Meeting.
Given the limited duration of single-shot nerve blocks, particularly in procedures such as TKA that demand sustained analgesia, this study addresses a key gap. The ACB offers motor-sparing benefits, favoring early mobility, but its duration when delivered as a single-shot is insufficient for long-term pain management. The use of peripheral nerve catheters to prolong ACB duration seeks to overcome this limitation, aiming to optimize pain control and reduce reliance on systemic opioids.
This triple-blinded, randomized controlled trial enrolled adult patients scheduled for primary unilateral TKA. Participants were assigned to one of two groups: one received a single-shot ACB with 0.25% bupivacaine and 4 mg perineural dexamethasone, and the other received a continuous ACB via catheter with 0.2% ropivacaine infusion over 50 hours. All patients followed a standardized multimodal analgesic regimen, which included IPACK block, periarticular infiltration, and oral medications (opioids, NSAIDs, acetaminophen, and muscle relaxants). The primary outcome was opioid use between 24- and 48-hours post-surgery, with secondary measures including total opioid consumption, pain scores, satisfaction, complications, and functional recovery.
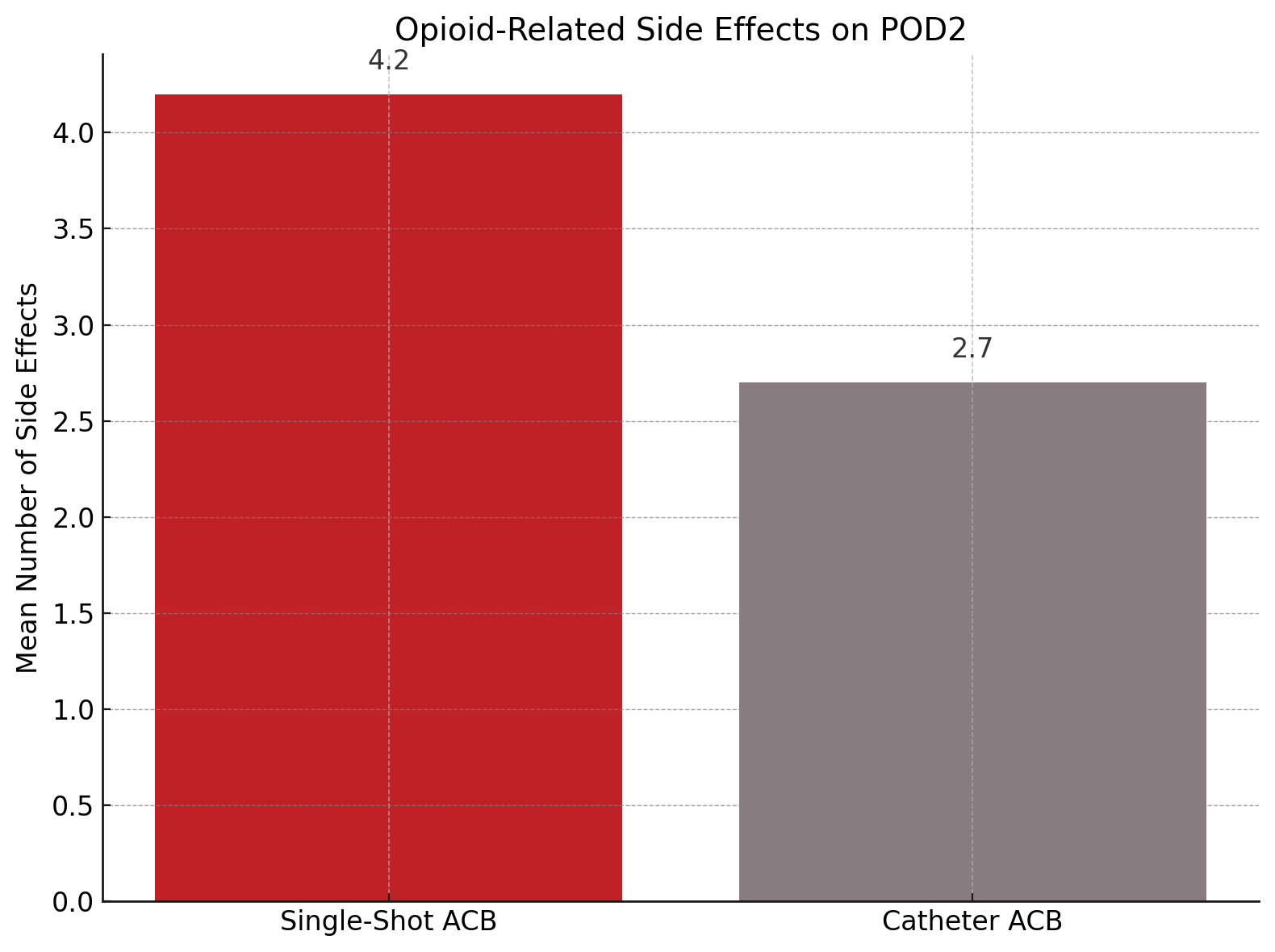
There was no statistically significant difference in opioid consumption during the targeted 24 to 48-hour window (catheter group: 43 ± 45.6 mg vs. single-shot group: 48.8 ± 37.5 mg, P = .213). Nonetheless, rest pain scores on postoperative day 2 were notably lower in the catheter group (mean difference -1.27; 95% CI, -2.35 to -0.2, P = .02). Additionally, fewer patients in the catheter group required rescue IV opioids (42.6% vs. 66%, P = .044), and they experienced fewer opioid-related side effects (mean 2.7 ± 2.7 vs. 4.2 ± 3.6, P = .0265). Other secondary outcomes, including patient satisfaction, block-related complications, hospital length of stay, and functional recovery, were comparable between the groups.
Limitations of this study include its performance within the framework of a robust multimodal analgesic protocol, which may have blunted detectable differences in opioid usage. Additionally, the exclusion of chronic opioid users and the controlled hospital environment may limit generalizability.
“Prolonging the duration of the ACB using peripheral nerve catheters did not result in reduced opioid consumption within the framework of a comprehensive multimodal analgesic regimen that included perineural dexamethasone, IPACK block, PAI, and continuous telemedicine-based pain consultation throughout the postoperative period,” the study authors concluded.
Reference:
Kim DH, Reisinger L, Liu J, et al. Continuous adductor canal catheter versus single-shot block with perineural dexamethasone for total knee arthroplasty: a randomized controlled trial. Presented at: Annual Regional Anesthesiology and Acute Pain Medicine Meeting; May 1-3, 2025; Orlando, FL.